
Key Summary
- Healthcare staffing challenges extend well beyond clinical roles because non-clinical teams support the operational infrastructure that makes care delivery possible.
- When non-clinical functions are understaffed or poorly designed, the impact quickly reaches patient access, reimbursement, compliance, and overall care quality.
- Clinical and non-clinical staffing should be treated as one connected workforce issue since breakdowns in support functions directly affect frontline performance.
- The strongest healthcare operating models combine reliable workflows, enabling technology, and integrated onsite and offshore support to improve resilience and efficiency.
When healthcare leaders talk about staffing shortages, the conversation usually starts with clinical roles. That makes sense. Nurses, physicians, and allied health professionals are essential, and the shortage of those people is real and serious.
But the staffing problem runs deeper than the bedside, and that is where most of the conversation stops.
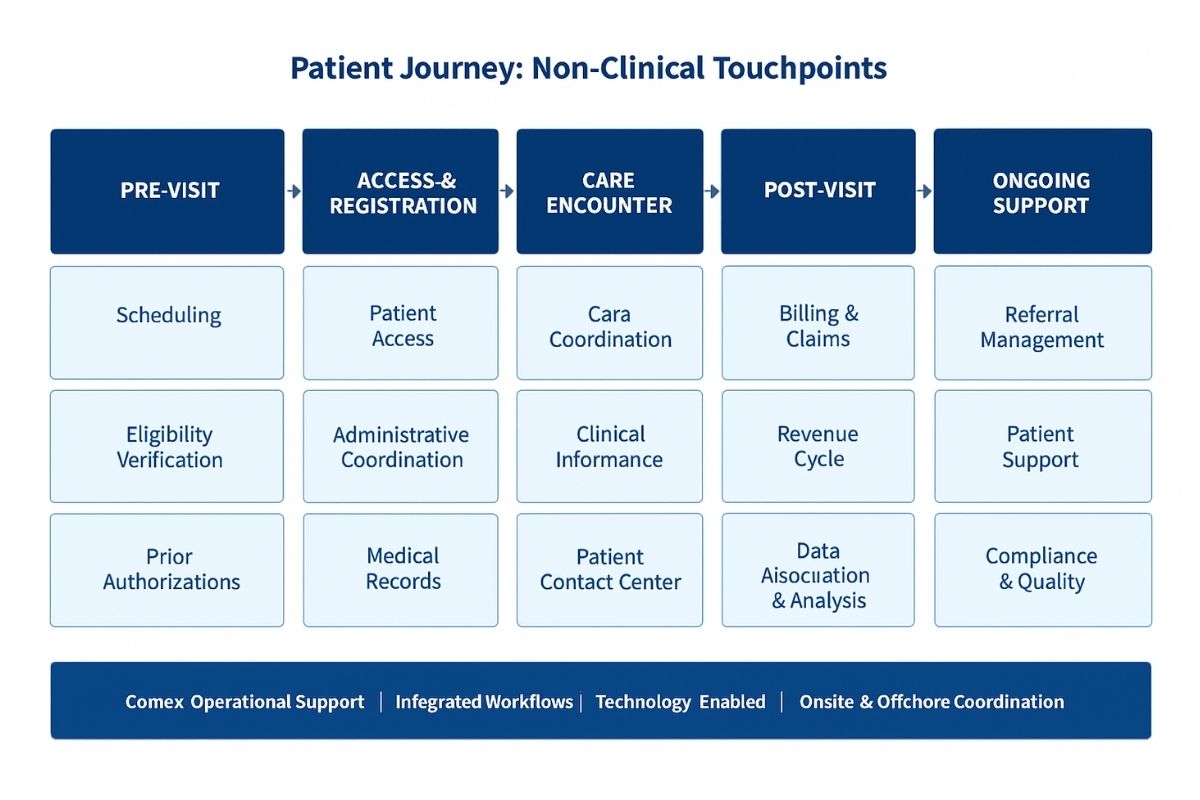
Healthcare organizations depend on non-clinical teams to function. Patient access, scheduling, revenue cycle, medical records, referrals, prior authorizations, billing, patient contact center operations, care coordination, clinical informatics, data abstraction and analysis, and administrative coordination are not background noise. They are the operational infrastructure that makes care delivery possible. When those functions are understaffed or poorly structured, the disruption does not stay in the back office. It moves upstream, and it moves fast.
The Operational Layer Is Not Optional
Every patient encounter depends on a sequence of work that happens before, during, and after clinical interaction. Appointments must be scheduled. Eligibility must be verified. Authorizations have to be secured. Documentation must flow accurately and on time. Claims must be submitted, tracked, and followed up on. Calls have to be answered. Records have to be placed cleanly between teams without friction or delay.
These are not administrative conveniences. They are load-bearing functions, and when any of them break down, the disruption compounds quickly.
Short-staffed scheduling teams degrade patient throughput. Understaffed prior authorization support delays treatment. Billing teams operating over capacity slow reimbursement cycles and drives denial rates up. Overwhelmed patient contact center staff create abandonment, patient frustration, and unresolved access barriers.
Quality care is defined by the right care, at the right time, in the right place, delivered by the right person. Operational support must be designed around the same standard. Work may not happen at the bedside, but it determines whether the bedside encounter can happen at all.
The solution to these problems is not simply adding a headcount. It is designing workflows that eliminate friction, integrating the right technology to automate repeatable tasks, and aligning offshore and onsite resources, so the operation runs as a connected system rather than a collection of isolated teams.
The Hidden Cost of Operational Gaps
Healthcare organizations tend to underestimate non-clinical understaffing because the damage is harder to see than an open clinical shift. But the consequences are measurable, and they accumulate.
Operational gaps slow intake, reduce throughput, delay claims, increase denial rates, create documentation bottlenecks, and introduce compliance exposure. They generate chronic overtime and manual rework. They push the organization into a reactive posture, managing exceptions instead of executing against a reliable process.
There is also a labor spillover problem that rarely gets accounted for. When support functions fall behind, work migrates to people who should not be doing it. Nurses absorb paperwork. Supervisors chase operational problems instead of developing their teams. Managers fill coverage gaps instead of driving process improvement. This disrupts top license equilibrium across the organization.
Highly trained clinicians and leaders pulled away from the work they can do, spending time on tasks that belong elsewhere in the workflow. That is expensive, and it is one of the most consistent drivers of burnout across the organization.
Clinical and Non-Clinical Staffing Are the Same Problem
One of the most consequential mistakes I see is treating these as separate workforce issues. They are not. They are interdependent components of the same operating model.
Clinical teams perform at their best when the systems around them are functioning well. They need clean handoffs, responsive operational support, accurate documentation flow, and process consistency. When any of those break down, clinicians absorb the impact immediately, even when the source of the failure is three departments removed.
Effective workforce strategy must account for the full operation. The question is not only whether the organization has enough nurses or coders or front-desk staff. The question is whether the entire support structure is engineered to sustain quality, efficiency, and growth. That requires earnest analysis of which roles require local presence, which functions can be standardized and optimized, and where integrated staffing models which combine technology, offshore capacity, and onsite coordination can improve performance without increasing operational complexity.
Building an Operating Model That Holds
The organizations that manage staffing pressure effectively are the ones that stop treating non-clinical functions as secondary. They recognize that operational infrastructure is a strategic asset, not an overhead category.
A stronger model is not built by filling open seats. It is built by designing reliable workflows, deploying the right technology to support repeatable functions, and integrating offshore and distributed teams in a way that creates genuine operational continuity. That includes functions like prior authorizations, scheduling coordination, medical billing, care coordination, clinical informatics, data abstraction and analysis, patient contact center operations, and administrative back-office work. These are areas where consistent process design and integrated staffing can drive measurable improvement in throughput, accuracy, and cost efficiency.
The objective is not to substitute for internal teams. It is to extend their capacity, reinforce their processes, and build resilience into the functions that the operation depends on every day. A well-integrated prior authorization team, for example, does not just process approvals. It reduces treatment delays, keeps revenue cycle velocity up, and removes a consistent volume of friction from the broader workflow.
Healthcare staffing problems go beyond clinical roles. The solution should go beyond them too and beyond staffing alone. Care delivery is only as strong as the operational model supporting it.
Final Takeaway
Healthcare organizations cannot achieve operational stability by focusing only on the clinical workforce. Stability comes from building an integrated support structure around care delivery — one that combines well-designed workflows, enabling technology, and the right mix of onsite and offshore resources. For leaders working to strengthen that foundation, Connext brings the operational expertise and staffing infrastructure to make it work.
Frequently Asked Questions
Healthcare staffing refers to the people and workforce structure that support care delivery across both clinical and non-clinical functions. Strong healthcare staffing is important because hospitals, physician groups, and healthcare organizations depend on the right mix of talent to maintain patient access, improve efficiency, protect revenue, and support better outcomes.
Healthcare staffing challenges go far beyond clinical roles because healthcare operations also rely heavily on scheduling, prior authorizations, billing, medical records, contact center support, care coordination, and revenue cycle management. When these functions are understaffed, delays, denials, administrative backlogs, and patient frustration can increase quickly.
Co-outsourcing improves healthcare staffing by allowing healthcare organizations to extend their teams without losing visibility or control. Instead of handing off an entire function to a traditional vendor, co-outsourcing creates a more integrated model where offshore or remote team members work as part of the broader operation, supporting consistency, accountability, and long-term scalability.
Outsourcing healthcare staff can be an effective strategy when it is done thoughtfully and aligned with operational goals. For many organizations, it helps address healthcare staffing shortages, expand capacity, reduce administrative burden, and improve turnaround times in areas such as scheduling, billing, prior authorizations, and patient support. The best results usually come from structured workflows, clear management, and strong quality oversight.
Virtual healthcare support can cover a wide range of non-clinical and administrative roles, including patient scheduling, referral coordination, eligibility verification, medical records support, billing assistance, care coordination, and contact center operations. This makes virtual healthcare support a practical option for organizations looking to strengthen healthcare staffing without adding pressure to onsite teams.
Virtual scribes help healthcare staffing by reducing documentation burden on providers and allowing clinicians to stay focused on patient care. By supporting charting and clinical note workflows, virtual scribes can improve efficiency, reduce administrative fatigue, and help organizations protect provider productivity in busy care environments.
Bilingual patient services are important in healthcare staffing because they improve communication, patient access, and the overall care experience for diverse populations. Healthcare organizations that offer bilingual patient services can better support appointment scheduling, patient inquiries, follow-up communication, and care navigation while reducing misunderstandings and improving patient satisfaction.
Revenue cycle management is closely tied to healthcare staffing because reimbursement performance depends on having the right people in place to manage eligibility checks, authorizations, coding support, claims submission, payment posting, denial follow-up, and account resolution. When healthcare staffing is weak in these areas, cash flow slows, denials rise, and operational strain increases.
Healthcare leaders should look for a healthcare staffing partner that understands both operational workflows and healthcare-specific requirements. That includes experience in co-outsourcing, strong management support, scalable recruiting, secure infrastructure, process discipline, and the ability to provide services such as virtual healthcare support, virtual scribes, bilingual patient services, and revenue cycle management support.
Start building your dedicated healthcare team with the right structure.
Connect with a Connext specialist to map out your approach.
Visit https://connextglobal.com/contact/ or email sales@connextglobal.com


